Breast Milk Jaudnice Vs Breast Feeding Jaundice
Breast milk jaundice
Hyperbilirubinemia - breast milk; Breast milk jaundice; Breastfeeding failure jaundice
Jaundice is a condition that causes the skin and whites of the eyes to turn yellow. There are two common problems that may occur in newborns receiving breast milk.
- If jaundice seen after the first week of life in a breastfed baby who is otherwise healthy, the condition may be called "breast milk jaundice."
- At times, jaundice occurs when your baby does not get enough breast milk, instead of from the breast milk itself. This is called breastfeeding failure jaundice.

Using bili lights is a therapeutic procedure performed on newborn or premature infants to reduce elevated levels of bilirubin. If blood levels of bilirubin become too high, the bilirubin begins to dissolve in the body tissues, producing the characteristic yellow eyes and skin of jaundice. Bilirubin also has an affinity for brain tissue, where it can accumulate and cause permanent brain damage.
Newborn jaundice (producing yellow skin) can have many causes, but the majority of these infants have a condition called physiological jaundice, a natural occurrence in the newborn due to the immature liver. This type of jaundice is short term, generally lasting only a few days. Jaundice should be evaluated by a physician until decreasing or normal levels of bilirubin are measured in the blood.
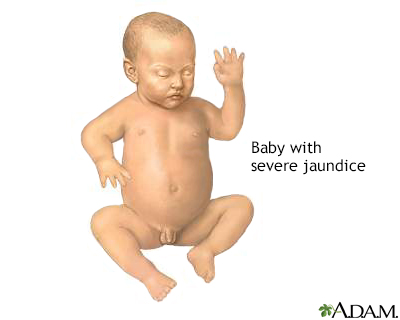
Jaundice is a yellow discoloring of the skin, mucous membranes, and eyes, caused by too much bilirubin (a breakdown product of hemoglobin made by the liver) in the blood. Jaundice is a condition produced when excess amounts of bilirubin circulating in the blood stream dissolve in the subcutaneous fat (the layer of fat just beneath the skin), causing a yellowish appearance of the skin and the whites of the eyes.
Causes
Bilirubin is a yellow pigment that is produced as the body recycles old red blood cells. The liver helps break down bilirubin so that it can be removed from the body in the stool.
It can be normal for newborn babies to be a little yellow between days 1 and 5 of life. The color most often peaks around day 3 or 4.
Breast milk jaundice is seen after the first week of life. It is likely caused by:
- Factors in a mother's milk that help a baby absorb bilirubin from the intestine
- Factors that keep certain proteins in the baby's liver from breaking down bilirubin
Sometimes, jaundice occurs when your baby does not get enough breast milk, instead of from the breast milk itself. This kind of jaundice is different because it starts in the first few days of life. It is called "breastfeeding failure jaundice," "breast-non-feeding jaundice," or even "starvation jaundice."
- Babies who are born early (before 37 or 38 weeks) are not always able to feed well.
- Breastfeeding failure or breast-non-feeding jaundice may also occur when feedings are scheduled by the clock (such as, every 3 hours for 10 minutes) or when babies who show signs of hunger are given pacifiers.
Breast milk jaundice may run in families. It occurs just as often in males and females and affects about a third of all newborns who get only their mother's milk.
Are your newborn baby's skin or eyes yellow? Is she extremely tired and doesn't want to eat? Your baby may have jaundice. Newborn jaundice happens when your baby has high levels of bilirubin in her blood. This yellow pigment is created in the body during the normal recycling of old red blood cells. The liver helps break bilirubin down so it can be removed from the body in the stool. Before a baby is born, the placenta removes the bilirubin from your baby so it can be processed by your liver. Right after birth, the baby's own liver takes over the job, but it can take time. Most babies have some jaundice. It usually appears between the second and third day after birth. Often babies get a screening test in the first 24 hours of life to predict if they are likely to develop jaundice. Your baby's doctor will also watch for signs of jaundice at the hospital, and during follow-up visits after your baby goes home. If your baby seems to have jaundice, the doctor will test the bilirubin levels in her blood. So, how do you treat newborn jaundice? Jaundice usually goes away on its own, so treatment is usually not necessary. If your baby's bilirubin level is too high or rising too quickly, however, she may need treatment. You'll need to keep the baby well hydrated with breast milk or formula. Feeding up to 12 times a day will encourage frequent bowel movements, which help to remove the bilirubin. If your baby needs treatment in the hospital, she may be placed under special blue lights that help break down bilirubin in the baby's skin. This treatment is called phototherapy. If your baby's bilirubin level isn't rising too quickly, you can also do phototherapy at home with a fiberoptic blanket that contains tiny bright lights. For most babies, it takes about a week or two for jaundice to go away. Very high levels of bilirubin, however, can damage a baby's brain. The good news is that this condition, called kernicterus, is almost always diagnosed long before bilirubin levels become high enough to cause damage, and phototherapy treatment will usually make it go away.
Symptoms
Your child's skin, and possibly the whites of the eyes (sclerae), will look yellow.
Exams and Tests
Laboratory tests that may be done include:
- Bilirubin level (total and direct)
- Blood smear to look at blood cell shapes and sizes
- Blood type
- Complete blood count
- Reticulocyte count (number of slightly immature red blood cells)
In some cases, a blood test to check for glucose-6-phosphate dehydrogenase (G6PD) may be done. G6PD is a protein that helps red blood cells work properly.
These tests are done to be sure that there are no other, more dangerous causes of the jaundice.
Another test that may be considered consists of stopping breastfeeding and giving formula for 12 to 24 hours. This is done to see if the bilirubin level goes down. This test is not always necessary.
Treatment
Treatment will depend on:
- Your baby's bilirubin level, which naturally rises during the first week of life
- How fast the bilirubin level has been going up
- Whether your baby was born early
- How your baby has been feeding
- How old your baby is now
Often, the bilirubin level is normal for the baby's age. Newborns normally have higher levels than older children and adults. In this case, no treatment is needed, other than close follow-up.
You can prevent the kind of jaundice that is caused by too little breastfeeding by making sure your baby is getting enough milk.
- Feed about 10 to 12 times each day, starting on the first day. Feed whenever baby is alert, sucking on the hands, and smacking the lips. This is how babies let you know they are hungry.
- If you wait until your baby cries, feeding will not go as well.
- Give babies unlimited time at each breast, as long as they are sucking and swallowing steadily. Full babies will relax, unclench their hands, and drift off to sleep.
If breastfeeding is not going well, get help from a lactation consultant or your doctor as soon as possible. Babies born before 37 or 38 weeks most often need extra help. Their moms often need to express or pump to make enough milk while they are learning to breastfeed.
Nursing or pumping more often (up to 12 times a day) will increase the amount of milk the baby gets. They can cause the bilirubin level to drop.
Ask your doctor before deciding to give your newborn formula.
- It is best to keep breastfeeding. Babies need their mothers' milk. Although a baby full of formula can be less demanding, formula feeding may cause you to make less milk.
- If the milk supply is low because baby's demand has been low (for example, if baby was born early), you may have to use formula for a brief time. You should also use a pump to help make more breast milk until baby is better able to nurse.
- Spending "skin to skin" time can also help babies feed better and help moms make more milk.
In some cases, if babies aren't able to feed well, fluids are given through a vein to help increase their fluid levels and lower bilirubin levels.
To help break down the bilirubin if it is too high, your baby may be placed under special blue lights (phototherapy). You may be able to do phototherapy at home.
Outlook (Prognosis)
The baby should recover fully with the right monitoring and treatment. The jaundice should go away by 12 weeks of life.
Possible Complications
In true breast milk jaundice, there are no complications in most cases. However, babies with very high bilirubin levels who do not get the right medical care can have severe effects.
When to Contact a Medical Professional
Call your health care provider right away if you are breastfeeding and your baby's skin or eyes become yellow (jaundiced).
Prevention
Breast milk jaundice cannot be prevented, and it is not harmful. But when a baby's color is yellow, you must have the baby's bilirubin level checked right away. If the bilirubin level is high, it is important to make sure there are no other medical problems.
References
Furman L, Schanler RJ. Breastfeeding. In: Gleason CA, Juul SE, eds. Avery's Diseases of the Newborn. 10th ed. Philadelphia, PA: Elsevier; 2018:chap 67.
Holmes AV, McLeod AY, Bunik M. ABM Clinical Protocol #5: peripartum breastfeeding management for the healthy mother and infant at term, revision 2013. Breastfeed Med. 2013;8(6):469-473. PMID: 24320091
Kaplan M, Wong RJ, Burgis JC, Sibley E, Stevenson DK. Neonatal jaundice and liver diseases. In: Martin RJ, Fanaroff AA, Walsh MC, eds. Fanaroff and Martin's Neonatal-Perinatal Medicine. 11th ed. Philadelphia, PA: Elsevier; 2020:chap 91.
Lawrence RA, Lawrence RM. Breastfeeding infants with problems. In: Lawrence RA, Lawrence RM, eds. Breastfeeding: A Guide for the Medical Profession. 8th ed. Philadelphia, PA: Elsevier; 2016:chap 14.
Version Info
Last reviewed on: 10/2/2020
Reviewed by: Neil K. Kaneshiro, MD, MHA, Clinical Professor of Pediatrics, University of Washington School of Medicine, Seattle, WA. Also reviewed by David Zieve, MD, MHA, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.

holstonsoollike80.blogspot.com
Source: https://www.mountsinai.org/health-library/diseases-conditions/breast-milk-jaundice
0 Response to "Breast Milk Jaudnice Vs Breast Feeding Jaundice"
Postar um comentário